Lenzer’s Tip Sheet for Journalists Covering Covid-19
Seek reliable sources:
Seek experts from the international List of Industry-Independent Experts, which is freely available to journalists Don’t be misled by experts with financial conflicts of interest. Information about The List is available here. Journalists are encouraged to nominate independent experts from all countries for consideration to be included on the List. Nominees are sent an application and a panel of four journalists/physicians will review each application.
Tools for assessing medical claims:
o HealthNewsReview: The premier source for journalists. HealthNewsReview provides structured critical appraisal of media reports on medical and health news, including covid-19. See the journalists’ toolkit available as a drop-down menu, which provides multiple tools including access to The List.
o Oxford COVID-19 Evidence Service: The Centre for Evidence Based Medicine in the UK; No woo or commercialism. Just science.
o National Center for Health Research: Provides updates on covid-19 and reports on conflicts-of-interest regarding vaccine development.
o Lown Institute Covid Tracker: Uses real-time changes in covid-19 to compare regions/countries.
o The BMJ: One of the top four medical journals in the world, the international medical journal provides all of its covid-19 reporting free-of-charge. Viewpoints vary and the site is useful to examine covid-19 from all angles.
o The Global Investigative Journalism Network provides additional guidance for reporting on covid-19 here.
o Worldometer and Our World In Data are useful data sites
Two reporting recommendations:
o #1: “Lockdown” is not one thing
§ Don’t try to assess whether lockdowns are “good” or “bad”/desirable or not: Lockdowns have many components: school closings (what ages?); masks (where, which types and under what conditions); use of fever hospitals vs quarantine; closing workplaces (which sorts); recreational shut downs (gyms, bars and enclosed spaces vs open-air parks, walkways etc.) See if you can find information about the specific components and their effects and not just whether a state, region or country is under “lockdown.” Evidence to support individual measures is sparse: avoid making assumptions.
§ Report harms as well as benefits of the various components of lockdown. Report downstream effects of lockdowns. All interventions, from social distancing to drugs can lead to harms: don’t ignore harms and “deaths of despair,” due to unemployment and evictions with their attendant increases in suicides, homicides, domestic violence, and drug and alcohol addictions. Track breaks in the food supply causing hunger. Many individuals are choosing to risk potential covid-19 infection over what are definite, immediate and serious threats to their lives and well-being in the present as they lose jobs and suffer evictions. To understand this, we have to drop political assumptions and listen carefully to the realities facing individuals.
o #2 Beware complexity
§ It is impossible to simply compare public health interventions in one region or country to another region or country and draw conclusions about causality. This is an incredibly complex area. Take the simple act of designating a death as “due to covid-19.” Example: 92-year-old woman is diagnosed with a mild case of covid-19. She is never hospitalized and does well for 3 months and dies. Did she die of covid-19 – or with covid-19?
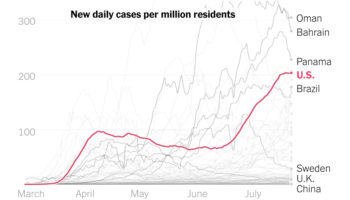
§ Or take the poor showing of the U.S. compared to other countries: Is it due to failure to initiate complete lockdown early – or is it due to the U.S.’s lack of a healthcare system available to all? Sweden implemented only certain components of lockdown and is currently doing far better than the U.S., according to this graph published in the New York Times. Are rising rates in the U.S. because the U.S. imprisons more people than any other country in the world? Could it be due to the extreme wealth gap in the U.S. with many homeless individuals compared to other OECD nations? Is the low rate of covid-19 due in Senegal due to care provided or because the average age in Senegal in 18.5 years and covid-19 deaths in such an age range is likely to be extremely low?
{kind=link}
§ Journalists must consider many factors when looking at mortality statistics, from the age of a population, to the number of people institutionalized, to weather and climate differences, to the presence or absence of a national healthcare system, to employment status, and much more.
§ Making assumptions about causality and deaths is fraught and answers may not be discernable in real time – or even for years to come.
Summary
Beware “official” reporting outlets in the U.S., and all countries. The current White House is side-stepping science, as is the case in at least a number of other countries – especially those with authoritarian governments. Even seemingly “independent” entities, from the U.S. Centers for Disease Control and Prevention, CDC, to the World Health Organization, WHO, have been compromised by financial conflicts of interest and their reports, while reliable in some instances, may not always be so.
Jeanne Lenzer
Independent medical investigative journalist, Frequent contributor, The BMJ, Bylines, Mother Jones, New York Times, Washington Post, Smithsonian. This page is reported for the Global Investigative Journalism Network